Part Four. Public Health Mobilization
16. A Path Analysis Model of Factors Associated with Child Immunization in Kano State
Baffa A. Umar and Mustapha M. Namadi
The National Program on Immunization is part of an international health scheme under the Primary Health Care (PHC) in Nigeria. The program was undertaken by the Nigerian government and ably supported by the United Nations Children’s Fund (UNICEF), the World Health Organization (WHO), and other agencies to immunize children against the six killer diseases: diphtheria, measles, pertussis whooping cough, poliomyelitis, tetanus, and tuberculosis; and to immunize pregnant women with tetanus toxoid to protect infants against neo-natal tetanus (Umar, 2004, 2006; Federal of Ministry of Health, 1988; Blum & Phillips, 1986; UNICEF, 1983; 1990, 1991, 1993, 1994, 2000, 2001, 2002). Immunization refers to the process and effect of producing immunity in children and pregnant mothers by administering attenuated vaccines. The child killer diseases are deadly, but preventable. If not controlled, the diseases can affect vulnerable and susceptible children with irrevocable consequences of mortality and morbidity.
Currently, Nigeria has one of the highest infant mortality rates in sub-Saharan Africa and particularly in West Africa, with 109/1000 live births (UNFPA, 2007). It is a paradox that this high death rate is prevalent despite Nigeria’s rich resource base as compared to lower rates in other countries with poor economic conditions, for instance, Guinea 97/1000, Senegal 79/1000, Togo 80/1000, and Mauritania 89/1000 (UNFPA, 2007, p. 87).
In fact, in Nigeria the problem of infant mortality due to the child killer diseases has been fluctuating as the health care provision and utilization faltered due to a number of problems (Blum & Philip, 1986; Federal of Ministry of Health, 1988; Babaniyi, 1990). Some of the problems include: (a) poor diseases notification system, (b) absence of sentinel surveillance system on monitoring the impact of diseases, (c) concentrating on vaccination for those over 1 year old, (d) unsatisfactory vaccine targeting, and (e) inadequate immunization coverage (Babaniyi, 1990). Already a record 80% immunization coverage against the child killer diseases was achieved in 1990 due to improvement in health delivery and political advocacy (Bondi & Alhaji, 1992). Still, a decline in immunization coverage was later experienced (UNICEF, 1994).
The Millennium Development Goals Report, 2006 indicates that “three out of four children are protected against measles, which still kills close to half a million children each year” (United Nations, 2006, p. 13). While “more children are surviving their first years of life [but] sub-Saharan Africa trails far behind” in the drive towards the attainment of Millennium Development Goals (United Nations, 2006, p. 12). It is becoming clear that sub-Saharan Africa and Nigeria in particular are lagging behind in achieving the Millennium Development Goals (MDGs). More needs to be done to attain the prescribed MDGs targets of eliminating preventable child diseases (Okonofua, 2005; United Nations, 2006).
In the family system, parents want their children to survive and to stay healthy. Therefore, it is expected that they would use all necessary means to ensure the survival of their children. The non-use of immunization services, then, suggests a problem. Non-use of immunization refers to the inability and/or refusal to utilize immunization services because of personal or other extraneous factors. Use of immunization refers to the acceptance and use of immunization services due to certain reasons. It also covers understanding, recognizing, and considering vaccination as the appropriate measure to prevent the six child killer diseases. There are complex factors that can facilitate acceptance, usage, or rejection of modern immunization by mothers or pregnant women, as is with the case with health utilization in general (Erinosho, 1998). Still, other factors are associated with use/non-use of immunization services. There are socio-cultural, economic, spatial (space/distance to a clinic), health, and religious factors associated with vaccination (Umar, 2004, 2006). It is important to identify these factors. The key variables on immunization usage are awareness, education, perception of mothers, and availability of vaccines. Other variables that are connected to immunization are:
- mothers’ proximity to the clinic,
- husbands’ influence,
- available money for clinic visits,
- poor consultation with mothers on immunization,
- social perception of immunization as a strategy for family planning, and
- side-effects of immunization.
This study focuses on mothers of children under five years old and pregnant/married women aged (15-45 years) who are the principal agents in childcare and immunization in the family.
Literature Review
The literature on patient compliance, which is associated with “usage,” indicates a connection to many factors. First, there is disparity in compliance in economically developed and developing countries. There are more cases of non-compliance with medical prescription in developing countries (Fraser, 1985). However, there are more chances for full compliance in cases with single-drug treatment; though there is an obvious difficulty in compliance as prescribed doses per day increase. When medical complications deteriorate, patients comply with medical prescriptions.
The literature in the health field, especially empirical findings, has demonstrated the positive and direct link between education and utilization of health services (Cairo Conference Paper, 1994; Caldwell, 1979; Muhuri, 1995; Levine, 1991). Using Nigerian data, Caldwell (1979) found that in addition it is a factor in mortality decline. Similar data from Matlab Bangladesh have further confirmed this relationship (Muhuri, 1995). Levine, (1991) indicates that mothers’ schooling is a predictor of risks to a child’s survival in Mexico. In Nigeria, differentials in maternal mortality across regions are attributable to disparities in education. For instance, because of differences in education, there are more maternal mortalities in the north than in the south of Nigeria; between mothers with little education and no education as well as between mothers in rural and urban centers (Cairo Conference Paper, 1994). Obermeyer (1993), in a comparative study of differential maternal care in Tunisia and Morocco, used logistic regression to determine the odds ratio and probability of utilizing prenatal services and hospital delivery. Like Caldwell (1979), she found education to be a strong factor in type and quality of maternal health care. In fact, higher formal education varies with improved health care utilization. Thus, as expected, there would be improved immunization as the mother is more educated. While this remains valid, Umar (2004, 2006), confirming Obermeyer (1993), found that both exposure to information on immunization through the radio and the availability of vaccines play a critical role in facilitating immunization. Other essential factors that play a key mediating role in supporting immunization are perception and education. The perceptual mind-set of mothers is central to making vaccination acceptable (Umar, 2004, 2006). Positive evaluation of outcomes of immunization, coupled with sustained motivation to prevent the occurrence of the six killer diseases, facilitates maternal acceptance of immunization. There are still other important factors in the background that may be associated with the entire process of immunization: proximity to the clinic, husbands’ influence, fear of potential side-effects, suspicion of family planning, and available funds for clinic visits.
Researchers are now looking beyond mere direct socialization influences to focus on multiple factors in maternal parenting that may be responsible for the child’s outcome (Kochanska, Aksan, Knack, & Rhines, 2004). Specifically, on immunization, Gage, Elizabeth, & Piani (1997) used Demographic and Health Surveys (DHS) for Niger (1992) and Nigeria (1990) and presented an important link between household structure and childhood immunization in Niger and Nigeria. Their analysis determined and developed the thesis that household structure is an important determinant of childhood immunization. This has wider connection with other economic variables in individual households and in sub-Saharan contexts as well (Gage, Elizabeth, & Piani, 1996). Other researchers have shown the way in which family structure, under the influence of parental cohabitation, can affect child outcome depending on economic resources, among other factors (Brown, 2004). At a more developmental level Papp, Cummings, & Schermerhorn (2004) have demonstrated a direct path link between mother’s distress and child adjustment. This may have implication for child immunization as marital distress in a patriarchal family in Nigeria can influence whether vaccination takes place depending on husbands’ permission (Cf Igun, 1988).
The field of medical sociology is heavily dominated by the theoretical focus of the Parsonian sick role (Parsons, 1951; Leoning Coovadia, Levine, & Kozzloff, 1978). Immunization, which falls within the rubric of health-related behavior, is part of preventive medicine (Umar, 2004). The Health Belief Model (HBM) is the theoretical perspective of this study (Kasl & Cobb 1966; Rosentock, 1966);
…the sick role is not an acceptable tool in preventive health analysis. The most logical tool of analysis is what is called Health at Risk: i.e. an individual may enter a process of health behavior when he/she is at risk of infection. Health behavior, here, ensues long before the infection. The possibility of infection makes a person to be a potentially ill person. So, because of this susceptibility, the pro-health behavior is cultivated to ensure healthy life through preventive measures. However, an individual may not know he/she is at risk due to illiteracy/ignorance, cultural influence etc. as opposed to when the infection sets in. Health at risk prepares a person to develop a particular behavior in interacting with health and, ill health behavior. This leads to what is called Health Belief Model (HBM). (Umar, 2006, p. 58)
Immunization as part of preventive medicine rests on the following premises:
- An individual places certain value on a given behavior interaction/action; i.e. if someone decides to partake in immunization, there is a feeling that he/she agrees with the sense of judgment for the action to be taken.
- By patronizing immunization there is a strong possibility that the person expects and even estimates a given result; i.e. there is the feeling that immunization would prevent the occurrence of a disease. Sick role, on the other hand, is based on illness; hence, it is not a health prevention exercise (Umar, 2006, p. 57).
According to Adeniyi (1991), the Health Belief Model “assumes that motivation is a necessary condition for action, because it selectively determines an individual’s perception of his environment,” thus providing the “psychological readiness” to act and patronize a particular health program:
- The action (e.g. getting vaccinated) “commands the individual’s sense of urgency;”
- The expected benefit of the health action is veritably seen as outweighing what may happen if the action is not taken;
- The resources and capability of the individual dictate what is to be done; and
- “The individuals’ psychological readiness to take action relative to a particular health condition.”
This can be determined by both the person’s perceived susceptibility and vulnerability to this particular condition, and by his perception of contracting the condition (Umar 2006, pp. 59-60).
Research Areas / Method
The research areas are in Warawa and Dawakin Kudu local government areas some 18 kilometres from Kano metropolitan along Maiduguri Road in northern Nigeria. The nearest dispensary to the villages is about 2 km from Mariri district. For any major health problem, the respondents would have to travel back to Kano (18 Km) or to Wudil (38 Km). There is easy access to the main Maiduguri Road; when there is urgent need for visiting the clinic/hospital, one would safely consider the fact that any failure to visit the clinic/hospital, when the need arises, may not be necessarily due to inaccessibility. The estimated population in the two villages is 6,000 people. However, in the suburbs, the areas are rural in nature. But modern developments are fast encompassing the two research areas because of their proximity to the Maiduguri highway and the Danladi Nasidi Housing Complex. The Hausa-Fulani dominates the research areas, and their religious belief is Islam.
Sample
There were 415 respondents for the research. The sampling method adopted was the total coverage sample. The target respondents were pregnant married women or nursing women with children 0-5 years old; the mothers’ ages ranged from 15-45. The respondents were selected because they are supposed to be directly involved in immunization. It is obvious that, unlike the general medical practitioners who physically study the child, in this research the mothers/pregnant married women are the units of analysis. They are socially closer to the children, and the children cannot speak for themselves. Hence, the mothers have a better opportunity to respond to the health issues pertaining to their children.
All individual households in the research areas were visited to select the eligible respondents. At the beginning, there was no specific sample size. Nevertheless, because the research focused on all households, there was the chance of covering all eligible respondents as in community-based studies. Even though this sampling technique is more difficult, because literally all the households were visited, it eventually resulted in a comprehensive survey that gives confidence for sound analysis and generalization. The data was a good representation of the general population at a time.
Data Collection
The data collection coincided with the time when the mothers were at home and were not busy at the farm. Seven research assistants, who lived in the villages, were recruited: Two males (university graduates) and five females (diploma certificate holders). It was not possible for the assistants all to be female degree holders in the areas. The selection was done in order to get research assistants who knew the area very well and, especially in the case of the females, who would be allowed to go into the households given the restrictions of entry in Muslim households. The research assistants were tutored on the nature of the research, its purpose, and the technical aspects of data collection. Luckily, the respondents had some idea of a research undertaking. With the permission of the village heads, there was easy access to the households. Also, the on-going house-to-house polio immunization was in progress when the data was collected. As a result, the female research assistants elicited responses from the mothers without many inhibitions. The males, as research supervisors, however, guided the females and organized the data collection accordingly. The research assistants translated the questions into Hausa language as they administered the questionnaires.
Because of the need to execute a meticulous work given the numbers of the households to visit, each household was marked and recorded taking into consideration the following: street, Primary Health Care (PHC) house number, household number and name of household head for easy reference, coordination, and compilation. A total of 415 respondents were found in the research areas. The respondents in Dawakin Kudu local government area constituted 60% (249), while that of Warawa local government area represented 40% (166) of the participants. Detailed questions on fertility, mortality, morbidity, socio-economic and cultural issues, and use of and perception on immunization were administered. Most of the questions were closed-ended with exhaustive choices to facilitate quantitative analysis.
The study (a) analyzed the use of the immunization services by mothers and pregnant women and, (b) determined and explained the factors influencing the use of the immunization services.
The dependent variable for the research is the use of immunization by the mothers. The sub-variables are regular use and irregular use of immunizations. The independent variables, on the other hand, as explanatory variables, are: (a) awareness, (b) education, (c) perception, and (d) availability of vaccines.
Even though the key variables for this research are awareness, education, perception, and use of immunization, there are also some alternative variables that are found to be relevant to the research; they are: (a) availability of vaccines, (b) mothers proximity to the clinic, (c) husbands’ influence, (d) availability of funds, and (e), poor consultation with mothers on immunization (Umar, 2004). Other antecedent variables considered are: (a) Perception of immunization as a strategy for family planning and (b) side-effects of immunization (Umar, 2004, 2006).
Research on Path Analysis
Path analysis, a technique for estimating the magnitude of the direct and indirect effects of certain variables on others, was employed in this research to examine immunization usage as well as the factors influencing the usage. Path analysis “is used to test the possibility of a causal connection among three or more variables” (Fraenkel & Wallen, 2000, p. 366). This is the part of correlational research that analyses associational relationships between variables without influencing the variables. In contrast to experimental research, variables in correlational research are not manipulated as in control and experimental design groups. The aim, rather, is to measure with a higher level of accuracy the predictable values of relationships between variables. The variable being used to predict the relationship is the predictor variable while the variable on which the prediction is made is the criterion variable. This is done through knowing the quantitative relationship between variables through the use of a correlation coefficient. Path analysis is a more superior analysis than other methods of determining causality or predictability (Fraenkel & Wallen, 2000).
Some of the basic issues being addressed by correlational analysis include:
- Is variable A associated with variables B and C?
- What is the direction of the relationship—positive, negative, direct, or indirect due to certain factors?
- What is the extent and predictive value of predictor variable B over criterion variable C?
- What are the wider relationships with the other variables under study?
- What kinds of general predictions and conclusions can be drawn based on the observed relationships between the variables?
Papp et al. (2004) developed pathways models on marital distress, maternal and paternal psychological symptoms, and child adjustments. Papp et al. (2004, pp. 368-384) found that:
- There was predicted direct relationship amongst family and child variables as demonstrated for both fathers and mothers.
- Maternal and paternal symptoms mediated the association between marital distress and child adjustment.
- Marital distress mediated the link between fathers’ symptom and child adjustment.
- However, direct pathway between mothers’ symptom and child adjustment remained.
Sullivan et al. (2004) adopted a path analysis model for predicting participation in health prevention program based on Health Belief Model (HBM). The objective of their study was to “determine which factors predict couple’s participation in premarital counseling.” Using HBM and the theory of reasoned action, they considered multiple factors associated with predictive behavior on participating in premarital prevention program.
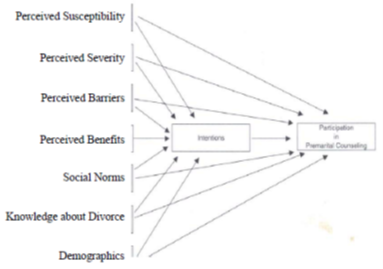
Adapted from Sullivan et al. (2004, p. 177) Social Norms
The above path analysis model is similar to the one adopted in this research. Just like in the research by Sullivan et al. (2004, pp. 175-194), the model affords the opportunity to determine pathways and relationships between variables that have predictive value over the use of immunization.
Findings
The pattern of effects between the dependent and independent variables was examined through direct and indirect decomposition. Table 1 presents the decomposition of the total effects of the predictor variables on the endogenous variable. It shows which variable mediate, the total of antecedent predictor variables, the portion of the total effect that is indirect (i.e. mediated by subsequent intervening variable), and the portion of the total effect (i.e. not mediated by an intervening variable).
| Indirect Effect | Direct Effect | Total effect | |
|---|---|---|---|
| Education | .001 | -.008 | -.007 |
| Awareness on Immunization | -.005 | .437 | .432 |
| Perception on Immunization | -.001 | -.312 | -.313 |
| Availability of Vaccines | -.051 | -.051 |
It should be noted that while the direct effect of a predictor variable may not have been significant, the calculation of the total effects of a predictor variable might reveal the existence of a statistically significant relationship. Examining total effects and their decomposition into direct and indirect components gives a more complete picture of the relationship amongst the variables in the model.
Model Specifications
The following equations have been derived from the proposed model of immunization usage based on hypothesized causal relationships. The symbols used in these equations represent the following variables:
X1 = Respondents’ Education
X2 = Awareness of Immunization
X3 = Perception of Immunization
X4 = Availability of Vaccines
X5 = Immunization Usage
P = Path Coefficient of Standardized Regression Coefficient
e = Error Terms or Source of Uncontrolled Error
X4 = P41 X1 + P42 X2 + P43 X3 + e4
X5 = P51 X1 + P52 X2 + P53 X3 + P54 X4 + e5
The symbol “e” indicates random disturbance caused by errors and by factors not explicitly included in the model. P is the regression coefficient for each explanatory
Basic Assumption Underlying the Path Analysis
- E(C1) = 0 sum of the error term is equal zero.
- E (ei ej) = 0 error terms are unrelated
- E (Xij ei) = 0 1. e.g. the error term for any equation is uncorrelated with the independent variable in that equation
Respondents’ education (X1), Awareness of Immunization (X2), and Perception of Immunization (P1) are exogenous variables, thus, variations are determined from outside the model. Therefore, their magnitude is equal to the error term. Availability of Vaccines (X4) is an endogenous variable and determined by Respondents’ Education (X1), Awareness of Immunization (X2), and Perception of Immunization (X3). Therefore, Availability of Vaccines (X4) is equal to the sum of Respondents’ Education (X1) multiply by the direct effect of Respondents’ Education on Availability of Vaccines multiply by the direct effect of Awareness (X2) multiplied by the direct effect of Respondents’ Perception of Immunization (X3), plus the error term.
Thus, each independent variable is determined by summation of each variable related to it through path coefficient (of the respective independent variable) with the dependent variable available.
Following the pattern established, Respondents’ Education multiply by the path coefficient between Respondents’ Education and Immunization Usage (P51), plus Awareness multiplied by the path coefficient between Awareness and Immunization Usage (P52), plus Perception multiplied by the path coefficient between Perception and Immunization Usage (P53) plus Availability of Vaccines multiplied by the path between Availability Vaccines and Immunization Usage (P54), will determine Immunization Usage.
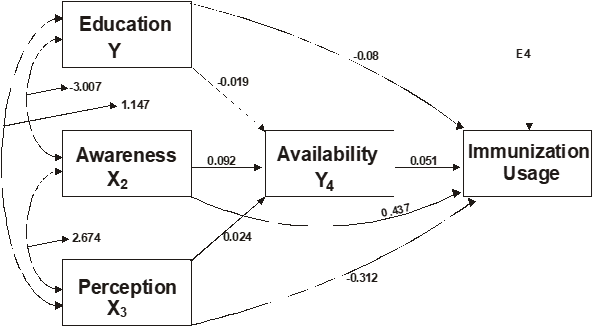
In the model, there is an interesting interlocking relationship between education, awareness, perception, and availability.
- Both mothers’ formal education [Y], (-0.08) and Perception [X3], (-0.312) have direct but negative relationships with immunization usage.
- There is, however, a strong relationship between mothers’ perception [X3], (-312) and awareness on immunization[X2], (2.674).
- There is equally a positive and direct path link between mothers’ perception[X3], and education [Y], (1.147).
- However, there is a negative path link between awareness on immunization [X2] and education (-3.007).
- In all, with the exception of formal education [Y], (-0.019), whenever availability of vaccines (Y4 ), mediates between awareness [X2], (0.092) and mothers’ perception [X3] (0.024), there is direct and positive link with immunization usage.
- Awareness [X2] has a direct path link with immunization usage, even though it also has indirect relationship with immunization usage through availability of vaccines.
Even though education is a major factor in determining health care utilization (Cairo Conference Paper, 1994; Caldwell 1979; Muhuri, 1995; Levine, 1991; Obermeyer, 1993), it has a weak direct link with immunization usage in this research. The major source of information on immunization in this research is the radio; this is associated with the level of exposure to knowledge on immunization services. Exposure to information on immunization, chiefly through the radio, accounts for acceptance and usage of immunization. Policy tools on immunization advocacy should take note of this development. Similar to this, Obermeyer (1993) found “in Tunisia, watching television weekly is associated with an increase in the likelihood of both prenatal care (OR = 1.85) and hospital delivery (OR = 1.64); a similar, if slightly weaker correlation for Morocco [OR = 1.72 and 1.49, respectively]”.
Conclusion
Despite the raging controversy over acceptability of immunization in northern of Nigeria where Muslims predominate (Umar, 2006), the level of acceptance and usage of immunization is high. There are multiple factors that mediate the efficacy of the immunization usage. Availability plays a critical role in the vaccination process. Future research should focus on the network of factors that mediate directly or indirectly to affect perception, awareness, and education as they affect immunization usage. Other variables mentioned in the paper may play a key role in certain contexts.
References
Adeniyi, J. D. (1991). The health problems of rural dwellers: A social-cultural perspective. Medicine Today – A Journal of Diagnosis, Treatment and Prevention, 1(3), 25-29.
Blum, D. & , M. (1986). An assessment of expanded program on immunization in Nigeria. New York, NY.
Bondi, F.S. & Alhaji, M.A. (1992). The E. P. I. in Bornu State, Nigeria: Impact on routine disease notification and hospital admissions. Journal of Tropical Medicine and Hygiene, 95, pp. 373 – 381.
Brown, S. L. (2004). Family structure and child wellbeing. Journal of Marriage and Family, 66(2), pp. 351-367.
Caldwell, J. C. (1979). Education as a factor in mortality decline: An examination of Nigerian data. Population Studies, 33(3), pp. 395-414.
Cairo Conference Paper, CCP. (1994). Nigeria concept paper for international conference on population and development ICPD. Cairo. Egypt.
Erinosho, O. A. (1998). Health Sociology. Ibadan: Sam Books.
Fraenkel, J. R. & Wallen, N. E. (2000). How to design and evaluate research in education. Boston, MA: McGraw-Hill.
Fraser, G. (1985). Compliance with medical therapy. World Health Forum (WHO) An International Journal of Health Development, 6(3), p. 64.
Gage, A. J., Elizabeth, S., & Piani, A. L. (1996). Household structure and child health in Sub-Saharan Africa. Demography and Child Health Surveys Analytical Reports, 1. Calverton, M.D. Macro International Incorporated.
Gage, A. J., Elizabeth, S., & Piani, A. L. (1997). Household structure and immunization in Niger and Nigeria. Demography, 34(2), pp. 295-300.
Igun, U. A. (1988) Medical Sociology Ibadan: Shaneson Limited C. I.in Child Development July /August Volume 75, Number 4 pp 1229–1242.
Kasl, S. A. & Cobb, S. (1966). Health behavior, illness behavior and sick role behavior. Arch Environ Health, 12, pp. 246-266.
Kochanska, G., Aksan, N., Knack, A., & Rhines, H. M. (2004). Maternal parenting and children conscience: Early security as moderator.
Leoning, V. E., Coovadia, H. M., Levine, S., & Kozzloff, M. A. (1978). The sick role: Assessment and overview, Annual Sociological Review, 4, 317-343.
Levine, R. et al. (1991). Women’s schooling and childcare in the demographic transition: A Mexican case study. Population and Development Review, 17(3), pp. 459-496.
Ministry of Health, Lagos.
Muhuri, P. K. (1995). Health programs, maternal education and differential child mortality in Matlab Bangladesh. Population and Development Review, 21(4), pp. 415-434.
Federal of Ministry of Health. (1988). NID’S, National Immunization Day’s: The Nigerian Experience. Lagos.
Obermeyer, C. M. (1993). Culture, maternal healthcare, and women’s status: A comparison of Morocco and Tunisia. Studies in Family Planning, 24(6), pp. 354-365.
Okonofua, F. E. (2005). Achieving the millennium development goals in Africa: How realistic. African Journal of Reproductive Health, 9(3), pp. 7-14.
Papp, L. M., Cummings, E. M., & Schermerhorn, A. C. (2004). Pathways among marital distress, parental Symptomatology, and child adjustment. Journal of Marriage and Family, 66(2), pp. 368-384.
Parsons, T. (1951). The social system. New York, NY: The Free Press.
Rosentock, I. M. (1966). Why people use health services. Milbank Men Fund, 44, pp. 94-127.
Sullivan, K. T., Pash, L. A., Cornelius, T., & Cirigliano, E. (2004). Predicting participation in premarital prevention programs: The health belief model and social norms. Family Process, 43(2), pp. 175-194.
Umar, B. A. (2004). A sociological study on the use of child immunization in Warawa and Dawakin Kudu local government areas in Kano State (Doctoral thesis, Bayero University, Kano).
Umar, B. A. (2006). Child immunization: Muslim reactions in Northern Nigeria. Kano, LOCATION: International Institute of Islamic Thought.
United Nations Children’s Fund (UNICEF). (2001). The state of world’s children 2001. New York, NY.
UNICEF. (2002). The state of world’s children 2002, New York, NY.
UNICEF. (1993). The state of world’s children 1993. London, England: Oxford University Press.
UNICEF. (1994). The state of world’s children 1994. London, England: Oxford Further Education College Press.
UNICEF. (1991). The state of world’s children 1991, Press Summary. New York, NY.
UNICEF. (1983). The state of world’s children 1982-1983. London, England: Oxford University Press.
UNICEF. (1990). First call for children: Convention on rights of the child/world declaration on the survival, protection and development of children.
UNFPA (2007) State of World Population 2007, Unleashing the Potential of Urban Growth, United Nations Population Fund, United Nations Systems.
United Nations. (2006). The millennium development goals report, 2006. New York, NY.
